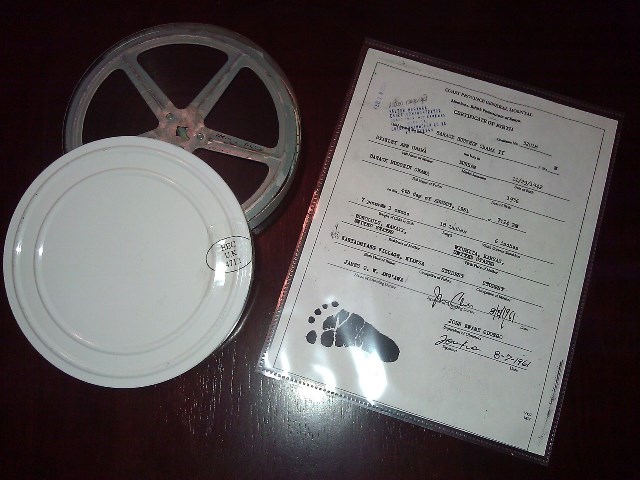
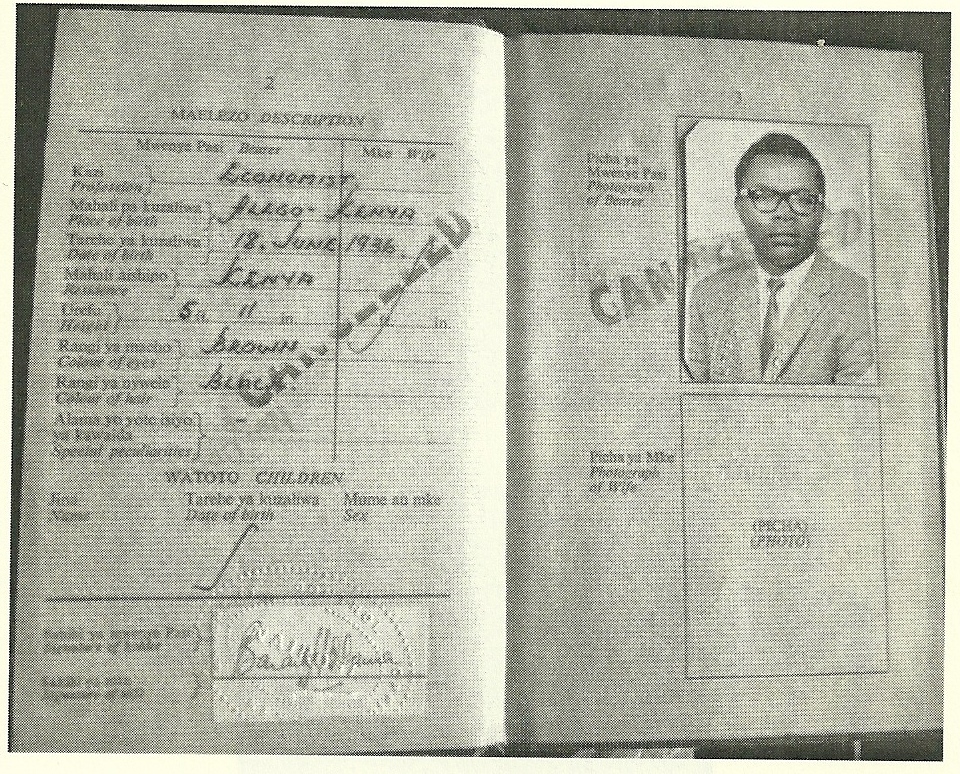
Barack Obama’s weight and length (as a newborn baby) were record in 1961 on his Coast Province General Hospital, Mombasa, British Protectorate of Kenya, certificate of birth. Additionally, a measurement defined (on the document itself) as “width between shoulders” was also recorded.

Skeptics have long indicated variants of the following:
1. “Width between shoulders” is not a measurement taken at birth.
2. “Width between shoulders” is a measurement which they’ve never heard of and, because they’ve never heard of it before, they believe that the birth certificate is somehow not authentic.
3. Even if “width between shoulders” was a genuine structure of measurement baby Barack Obama’s is listed as “6 inches” and that is too large for a newborn baby.
There have also been countless and innumerable supplementary speculations (reckless speculations) regarding the measurement which I wont waste time going into but, for example, there was one about “width between shoulder” being a measurement used only for animals and not for humans.
As you may know, the doctor who delivered baby Barack Hussein Obama II was James Oyunga William Ang’awa.

Its should also be noted that Doctor Ang’awa lived in the same neighborhood, Upper Hill, in Nairobi with Barack Obama Sr. during the mid-to-late 1960s 1970s and up thru Obama Sr.’s death in 1982. (See Ogosia, Kenneth. “You are forgiven, judge tells her father’s killer.” The Nation. January 30, 2010.)
In the year 1951, ten years before baby Barack Obama was born at the Coast Province General Hospital in Mombasa, Dr. Ang’awa published a paper entitled, “RUPTURE OF THE UTERUS IN EAST AFRICA: A Note on its Incidence and Aetiology in Women of the Kikuyu Tribe.” A more detailed version of the paper, known simply as Rupture of the Uterus, was also published the East African Medical Journal the following year in 1952
In the 1951 paper, page 1030, Dr. Ang’awa discusses “Shoulder presentation” –
“Group 2. Shoulder presentation; 8 cases. This group was subdivided as follows : (I) Spontaneous rupture with shoulder presentation. (“Neglected transverse.”) (2) Rupture discovered after obstetric manipulations in hospital. (3) Rupture discovered at autopsy, after obstetric manipulations in hospital.”
It appears that Ang’awa’s paper attempted to determine factors and causes of uterine rupture and ventured to draw conclusions of how and why the uterus is ruptured. All cases of ruptured uterus were divided into six (6) groups and some groups were subdivided. One group of the pregnant women consisted of those who exhibited signs of ‘Shoulder presentation’.
Moreover, the ‘Shoulder presentation’ group was subdivided into the following three (3) categories:
1. Spontaneous rupture with shoulder presentation. (“Neglected transverse.”)
2. Rupture discovered after obstetric manipulations in hospital.
3. Rupture discovered at autopsy, after obstetric manipulations in hospital.
Shoulder presentation is a malpresentation of the fetus in which the shoulder, and sometimes the arm itself, is positioned towards the mother’s pelvic inlet of the birth canal. Typically an infant cannot, outside of a cesarean section being performed, be delivered in such a position (i.e., malpresentation).
It is presumable and not unlikely that shoulder width measurements (i.e., ‘width between shoulders’) of newborn babies became common practice, if not routine, by doctors such as Ang’awa in the Colony and Protectorate of Kenya in efforts to learn more about the following:
A. ‘Shoulder presentation’ and factors, circumstances, and influence that contributes to the causes of.
B. ‘Rupture of the uterus’ (more commonly known as “uterine rupture”) and factors, circumstances, and influence that contributes to the causes of.
C. ‘Neglected transverse’ (more commonly known as “Neglected transverse lie”) and factors, circumstances, and influence that contributes to the causes of.
1951. James Ang’awa. "RUPTURE OF THE UTERUS IN EAST AFRICA: A Note on its Incidence and Aetiology in… by Lucas Daniel Smith
A somewhat similar condition known as “Shoulder Dystocia” occurs when a fetus/infant cannot be delivered because the shoulders are too wide to pass through the mother’s Pubic symphysis.
There are published studies, similar to doctor Ang’awa’s paper, on ‘Shoulder Dystocia’ in which doctors, attempting to determine risk factors and causes of, have taken ‘shoulder width’ measurements. The following study was originally located by Bruce Steadman on 05.28.2012 and posted on the InspectorSmith Forum- “The ‘Lucas Daniel Smith, Obama Kenyan Birth Certificate’ indicates that Barack Obama was born a short, broad-shouldered, slightly-less-than-average weight baby, but NOT some improperly proportioned ‘dwarf’ as some ‘forgery-promoting’ individuals have claimed.” – and that study is discussed below:
Verspyck, Eric; Gofinet, François; Hellot, Marie F.; Milliez, Jacques; Marpeau, Loïc. “Newborn shoulder width: a prospective study of 2222 consecutive measurements.” British Journal of Obstetrics and Gynaecology. Vol 106, pp. 589-593. June, 1999.
Page 589:
“Population A total of 2222 newborn shoulder width measurements were performed and 22 cases of true shoulder dystocia occurred during the study period.”
“Methods Newborn shoulder width measurements were reviewed and correlated with maternal age, parity, nonpregnant weight, weight gain during pregnancy, height, race, fasting glucose and one hour glucose levels, gestational age, birthweight and sex of the neonate. A receiver-operating characteristics curve was constructed to evaluate newborn shoulder width as a test for predicting shoulder dystocia.”
“Results The mean newborn shoulder width was 122.06 mm (10.50 SD). Stepwise multiple regression showed that newborn shoulder width was significantly associated with birthweight (P < 0.001), parity (P = 0.04), and nonpregnant weight (P = 0.04). We estimated that the best cut off for shoulder dystocia prediction was a newborn shoulder width measurement with a low false positive rate (< 10%) in association with a high sensitivity rate. Therefore, newborn shoulder width measurement > 140 mm was selected. This measurement should have a low sensitivity of 27.27%, a specificity of 91.82%, a positive predictive value of 4.02%. and a negative predictive value of 99.01% for shoulder dystocia prediction. Nevertheless, birthweight > 4000 g should have a better predictive value retrospectively for shoulder dystocia.”
“Conclusions Newborn shoulder width measurement, which is strongly correlated with birthweight, still remains a poor predictor for shoulder dystocia, even when this evaluation is correct antenatally.”
Between more than 2000 shoulder width measurements the mean average reported was 122.06 mm (millimeters) which is the equivalent of 4.826 inches.
The study also expresses, on page 590, that, “Ethnic variations were studied after comparaisons between Caucasians, North African, black and Asian groups. Shoulder dystocia was defined as manoeuvers that were required to deliver the shoulders in addition to downward traction of the fetal head and episiotomy……The mean newborn shoulder width was not different between white infants [121 mm (10.1), 52.08%], North African infants [122.2 mm (10.8), 14.84%], black infants [120.9 mm (10.6), 14.25%] and Asian infants [121.2 mm (1 1.9), 8-9%].”
Newborn baby Barack Obama’s width between shoulders measurement was recorded on his 1961 Kenyan birth certificate as “6 inches” which is the equivalent of 152.400 mm (millimeters).
Difference between the above study’s means average and Obama’s measurement: 30.34 millimeters or 1.194 inches.
In my opinion I don’t see how a difference of 1.194 inches would fall outside of the standard deviation of a mean average of 4.826 inches.
To calculate the shoulder width standard deviation, we’d need to compute the difference of shoulder width measurements from the mean average and then square the result of each.
Each of the more than 2,000 shoulder width measurements are NOT provided so we cannot calculate the standard deviation.
However, again, in my opinion, I don’t see how the difference noted above would fall outside of what is known as standard deviation. If anyone reading has evidence to the contrary I welcome and implore you to post that same in the comments section at the foot of this blog report.
Moreover, I don’t see how a study of a little more than 2000 newborn babies, all within the country of France, granted ethnic variations (within France) were included in the study, suffice to epitomize all newborns in a world with a population of nearly 7 (seven) billion where, in the United States of America alone, approximately 4 (four) million babies are born each year. The study is a little to ‘PC’ (politically correct) for me.
I prefer Dr. Ang’awa’s paper in which, notwithstanding that the paper is void of shoulder width measurements(!), he seems to contend that ethnicity and culture are applicable and are factors.
1999. "Newborn shoulder width: a prospective study of 2222 consecutive measurements." British Jo… by Lucas Daniel Smith
I haven’t been able to locate or acquire any other hospital birth certificates which request or provide a measurement for “width between shoulders”. However, I do have in my possession a hospital birth record titled “NEWBORN SUMMARY” which requests a similar sort of measurement listed as a Chest Circ. (i.e., Chest Circumference).
In closing I want to state here for the record that fetus/infant shoulder width has proven, overwhelmingly, to be worthy of attention. Depending on the width of the fetus’/infant’s shoulders normal delivery of the baby may not be possible and could potentially, if not outrightly and aggressively, become life threatening for both the mother and the baby.
In some extreme cases, after all other methods to manipulate the baby have failed or are no longer (or never were) an option, a procedure known as a Cleidotomy is performed. The collarbone (clavicles) is cut/divided by a surgeon to make the shoulders less broad. Its a risky operation any typically not performed on living babies outside of there being no other operable alternatives.
Please exercise your free speech in the comments section below. There are no stipulations of political correctness on this blog. Speak your mind, give us your thoughts, both objective and subjective. Share your ideas, hunches, inklings or your expertise. Please provide recommendation and corrections if you spot errors in fact within the blog report. Lastly, remember that posting a comment is much like casting a vote, so please do so.


")

")

")


 Franklin Delano Roosevelt, the 32nd President of the United States of America was elected four (4) times, i.e., 1932, 1936, 1940 and 1944.
Franklin Delano Roosevelt, the 32nd President of the United States of America was elected four (4) times, i.e., 1932, 1936, 1940 and 1944.